Administering Deflux
Endoscopic treatment with Deflux takes about 15 minutes on an outpatient basis and usually allows the child to go back to normal activities the day after it’s done.1
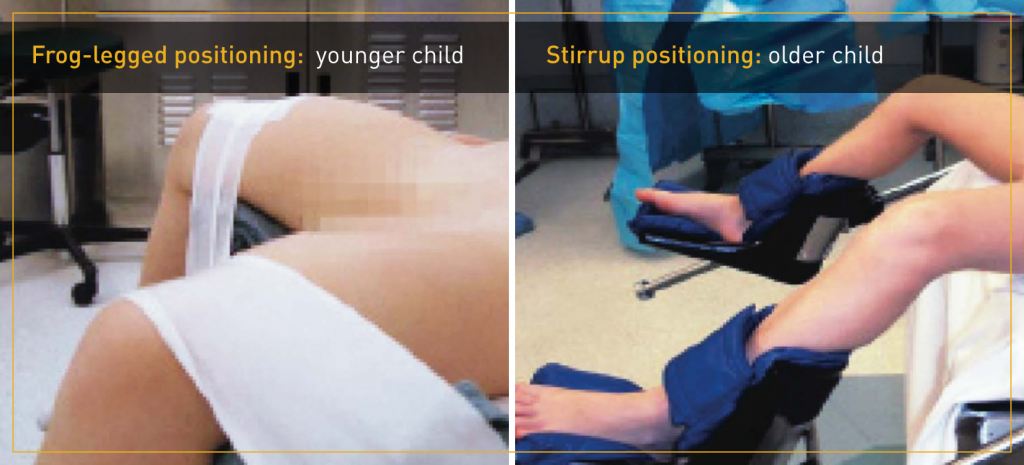
The patient is first placed under general anaesthesia. With the patient properly positioned, a cystoscope is inserted, and the Deflux needle is inserted in the working channel of the cystoscope. Deflux is injected submucosally in the urinary bladder in proximity to the ureteral orifice or in the distal ureter. The injection of Deflux creates increased tissue bulk thereby providing coaptation of the distal ureter during filling and contraction of the bladder. The dextranomer microspheres are gradually surrounded by host connective tissue at implant site.2
Deflux is injected according to the recommended technique, after which the needle and cystoscope are withdrawn, and postoperative care is given.
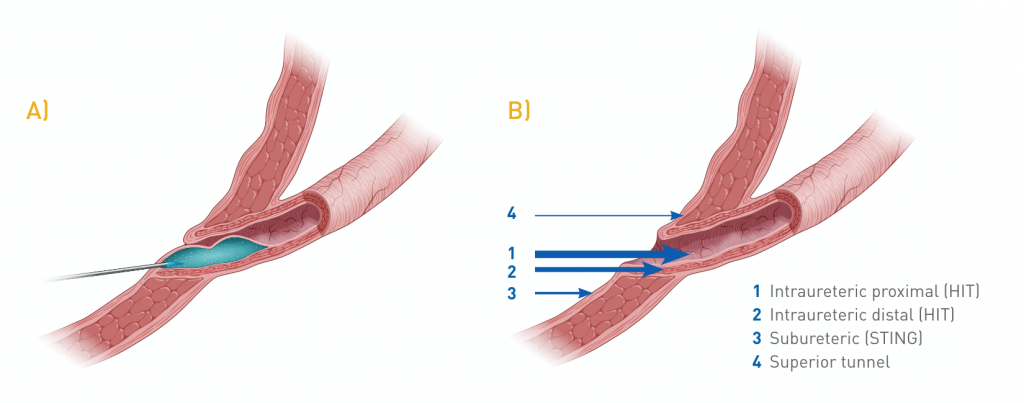
Double HIT technique
Techniques for administering Deflux have evolved over time, from subureteric injection (STING) to single intraluminal HIT (Hydrodistention Implantation Technique) to tandem proximal and distal intraluminal injection sites (Double HIT).3 In recent years, the Double HIT technique (Figure 1) has increasingly become the most commonly performed technique for correction for VUR by paediatric urologists in the United States. In 2014, a study showed 92% of Deflux procedures use the Double HIT technique which has demonstrated higher efficacy rates.4
Double HIT methodology3
The Double HIT method is currently achieving the highest rates of success. The bladder is filled to less than half capacity to permit visualization of the ureter and avoid tension within the submucosal layer of the ureter secondary to overdistension. The needle is passed into the ureteral orifice (UO) and inserted at the mid ureteral tunnel at the 6 o’clock position. Sufficient bulking agent is injected to produce a bulge, which initially coapts the detrusor tunnel, while a second implant within the most distal intramural tunnel leads to coaptation of the UO. HD is performed after each injection to monitor treatment progress; when HD ceases to dilate the UO, appropriate coaptation has been achieved.
Figure 1. Double HIT Technique5